Blog
May 14, 2026

Nearly one in seven Americans now live in what researchers call a pharmacy desert. That's roughly 50 million people, according to a 2024 Ohio State University study, and the number has climbed since.
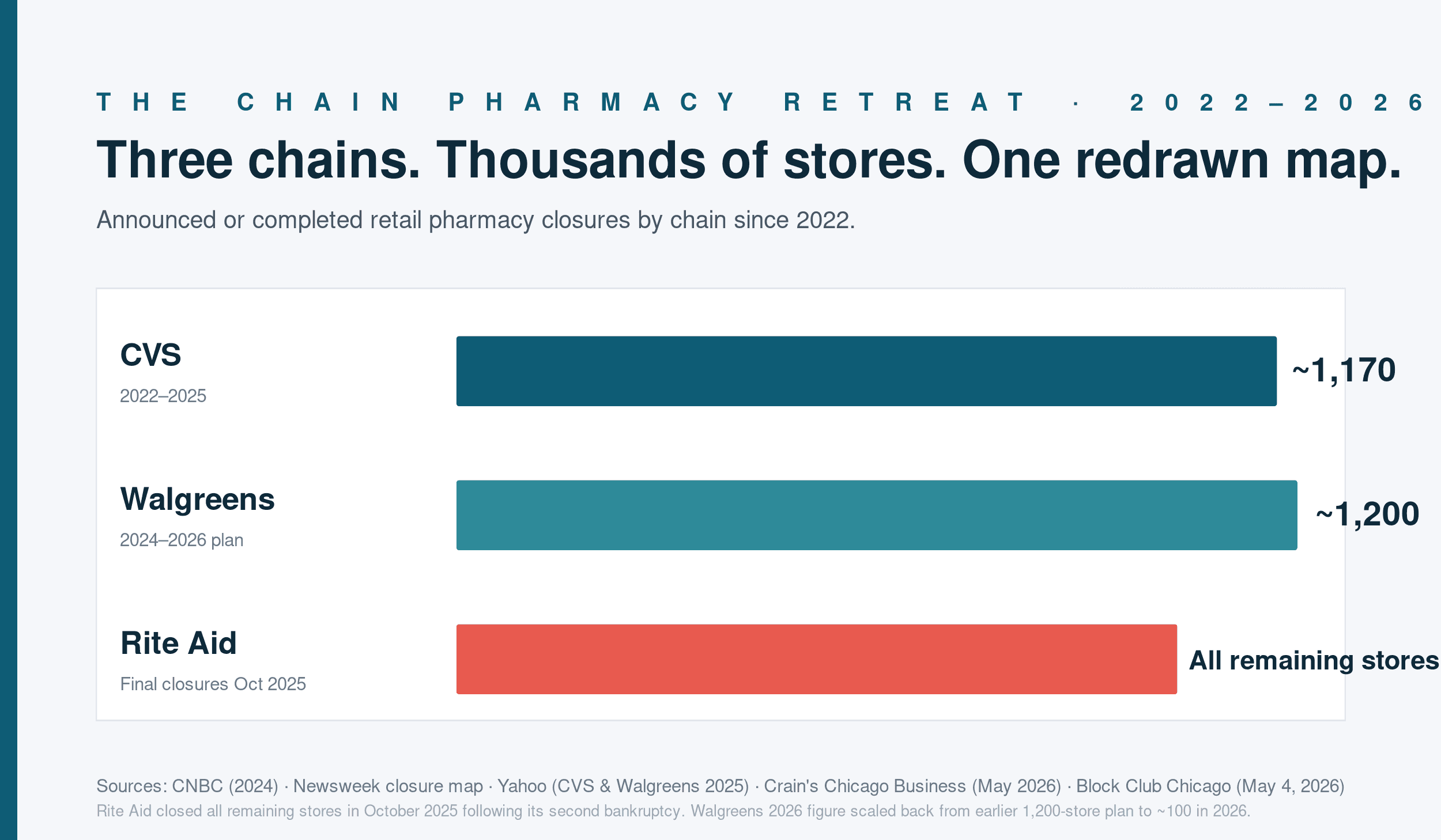
After 63 years in business, Rite Aid closed all of its remaining stores in October 2025 following its second bankruptcy. CVS shuttered about 270 stores in 2025, on top of roughly 900 closures between 2022 and 2024. Walgreens expects to close under 100 more locations in 2026, scaled back from its original announcement of 1,200 closures over three years. The chains made these decisions for their own reasons. The communities left behind don't get to vote.
For pharmacy owners, operators, and staffing leaders, the desert map is more than a policy concern. It's a strategic one. Where chains pull out, demand doesn't disappear. It shifts. And the pharmacies that pick up the slack need staffing models that match the new reality.
What pharmacy deserts actually look like on the ground
A pharmacy desert is generally defined as a community without a drugstore within a 10-mile radius. The University of Southern California's pharmacy desert map shows the problem is concentrated in rural counties, low-income urban neighborhoods, and communities of color. According to Ohio State University research, residents of nearly half the nation's counties live in one.
The health consequences are well-documented. People in pharmacy deserts are less likely to take their medications, more likely to skip doses, and more likely to experience worse cardiovascular outcomes. When a 30-day fill requires a 90-minute round trip, adherence drops. That's geography doing what geography does, with no moral failing required on the patient's part.
The opportunity for independents and small chains
When a CVS or Walgreens closes, the nearest independent pharmacy often absorbs the patient panel. That's good for the independent's revenue, but only if the operation can scale to meet it.
The math is unforgiving. A pharmacy that handled 200 scripts a day cannot smoothly handle 350 with the same staff. Wait times grow, errors climb, technicians burn out, and pharmacists start looking for jobs that don't end at 9 PM. The pharmacies that successfully absorb a competitor's closure plan their staffing response in advance, not after the first wave of new patients walks in the door.
Three patterns show up consistently among independents that absorb a closure well.
They upskill their existing staff and invest in continuing education. Technicians can do more than they used to. Most states now allow technician-administered immunizations, and many allow techs to play a larger role in compounding, intake, and patient counseling support. Pharmacies that fund certifications, support specialty training, and develop senior tech roles internally can stretch existing capacity in a way that purely external hiring cannot.
They build a per diem and relief bench before they need it. A relief pharmacist who knows your workflow and your patient base is worth ten resumes from people who don't. Pharmacies that maintain ongoing relationships with relief and per diem pharmacists can ramp coverage quickly when demand surges. Pharmacies that are starting cold spend the first month just finding people.
They get the word out fast. When a chain closes, patients don't always know which pharmacies are accepting transfers. Independents that get a clear message out, through local press, social media, or community partnerships, capture more of the displaced patient base than those that wait to be found.
The staffing model question
Pharmacy deserts complicate the standard staffing playbook. The places where coverage is hardest to find are also the places that need pharmacies most. Rural Mississippi is not Jackson. A small town in Eastern Oregon is not Portland.
This is where flexible staffing models, used well, become a public health tool, not just an operational one. A pharmacy that can pull in a relief pharmacist for two days a week may be the difference between staying open and adding to the desert map. A hospital pharmacy that can use per diem coverage during seasonal surges keeps its inpatient pharmacist from rotating through a 14-day stretch.
There's a tendency to talk about per diem and relief pharmacy as a backup option. In communities where the alternative is closure, it's the primary one.
There's a quieter piece of the rural staffing equation: the semi-retired pharmacist. In small communities where agency relief is hours away and the new-grad pipeline is thin, owners are increasingly calling back pharmacists who retired in their early 60s or stepped down to part-time. The deal is direct. Two or three shifts a month, paid above the historical local rate, with the schedule shaped around the pharmacist's life. The income bump matters, and the work is often genuinely meaningful to someone who knows the patient base from decades of practice. This won't solve the long-term workforce shortage. In the smaller deserts, though, it's frequently what keeps the doors open.
What this means for the next 18 months
The chain pullback isn't finished. Walgreens will continue closing stores through 2026 and into 2027. Independent acquisitions are picking up where Rite Aid's footprint used to be. The map will keep redrawing.
For pharmacies that want to be part of the answer, three things are worth doing in the next quarter.
Map your service area. Know where the nearest closures have been and where the next ones might happen. Walgreens publishes its closure announcements. Patients of closing stores need somewhere to go. That somewhere can be you, if you're prepared.
Stress-test your staffing model. If your script volume increased by 40 percent over six months, could you handle it? What would break first? Build the answer now.
Treat per diem as core, not contingency. The pharmacies that are quietly absorbing closures are also the ones with the deepest benches. That's not a coincidence.
The desert map is a map of opportunity for the pharmacies that can show up. It's also a map of patients who need someone to. Both things are true at once.